Vitamin D Realities
Evidence-Based Insights on Health, Deficiency, and Supplementation
SUPPLEMENTS
2/4/20265 min read
Vitamin D Realities: Evidence-Based Insights on Health, Deficiency, and Supplementation
You probably hear a lot about vitamin D — that it’s a miracle cure, a must-have supplement, or something you only get from sunbathing. Cut through the noise: vitamin D supports bone health, muscle function, and immune responses, but its benefits, optimal levels, and risks depend on your situation, not on blanket claims.
Knowing whether you need more vitamin D, how to get it safely, and when supplementation helps will protect your health more than any trend-driven routine.
This post will clarify what vitamin D actually does, how deficiency and excess affect you, and how to make practical choices about sun exposure, diet, and supplements so you can act with confidence.
Key Takeaways
Vitamin D plays specific roles in bone, muscle, and immune health.
Not everyone needs supplements; testing and context matter.
Both deficiency and excess can cause harm, so aim for balanced intake.
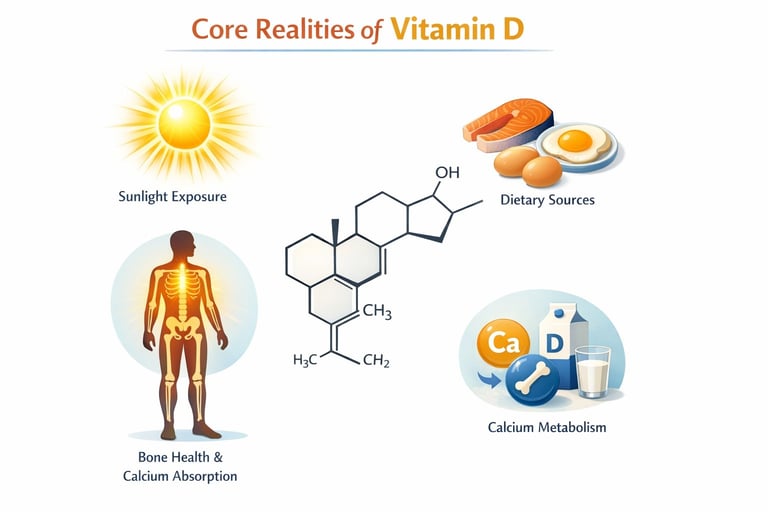
Core Realities of Vitamin D
Vitamin D exists in specific chemical forms, is made or obtained from clear sources, acts through defined metabolic steps, and has measurable clinical consequences when levels fall or rise. You will learn what each form does, how your body processes it, which health issues link to deficiency, and what intake or testing targets guide safe supplementation.
Forms and Sources of Vitamin D
Vitamin D appears mainly as vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). D3 comes from skin synthesis after UVB exposure and from animal-derived foods like cod liver oil; D2 comes from some fungi and fortified foods.
Fortified milk and other fortified foods commonly supply dietary vitamin D in many countries. Over-the-counter vitamin D supplements contain either D2 or D3; D3 is generally more effective at raising and sustaining blood levels.
Your skin production depends on latitude, season, time outdoors, clothing, and skin pigmentation. Absorption from food or supplements requires dietary fat and normal intestinal function, because vitamin D is fat-soluble. Both forms are transported to the liver for initial conversion before becoming active.
Biological Role and Functions
Your liver converts vitamin D to 25-hydroxyvitamin D (calcifediol), the main circulating form measured to assess vitamin D status. The kidney (and some other tissues) converts 25(OH)D to the active hormone calcitriol (1,25-dihydroxyvitamin D), which binds the vitamin D receptor in many cells.
Calcitriol enhances intestinal absorption of calcium and phosphate, supports bone mineralization, and influences muscle function. It also modulates immune responses, cell proliferation, and some endocrine pathways such as parathyroid hormone regulation. Low calcitriol elevates parathyroid hormone, which can increase bone resorption and reduce bone density.
Vitamin D Deficiency and Associated Conditions
Low blood levels of 25(OH)D associate with rickets in children and osteomalacia in adults—conditions of defective bone mineralization. Chronic insufficiency contributes to lower bone density and increased osteoporosis risk, with higher fracture likelihood. Muscle weakness and falls are common clinical features of deficiency.
Secondary hyperparathyroidism can result from inadequate vitamin D, driving calcium mobilization from bone. Rare genetic disorders such as familial hypophosphatemia or defects in vitamin D metabolism may require active forms like calcitriol rather than standard supplements. You should suspect deficiency when patients report bone pain, weakness, or have risk factors like limited sun exposure or malabsorption.
Vitamin D Intake and Requirements
Public guidelines target blood 25(OH)D concentrations as the primary marker of adequacy; many agencies consider ≥20 ng/mL (50 nmol/L) sufficient for most bone health outcomes, though some recommend higher targets for specific populations. Recommended dietary intakes vary by age, pregnancy, and health status; common daily doses range from 400–800 IU, with higher therapeutic doses used under medical supervision.
Supplement selection matters: cholecalciferol (vitamin D3) raises serum 25(OH)D more predictably than ergocalciferol (vitamin D2). Monitor blood levels if you take high-dose supplementation, have malabsorption, or chronic kidney disease. Avoid excessive doses without medical advice because very high vitamin D can cause hypercalcemia and related harms.
Vitamin D Supplementation: Benefits, Risks, and Nuances
Supplementing with vitamin D affects bone health, muscle function, immune response, and certain disease risks; dose, baseline level, and individual factors determine benefit and safety. Pay attention to form (D3 vs D2), daily dose, and monitoring to balance effects and avoid harm.
Benefits and Effectiveness for Different Populations
If you are deficient (25‑OH vitamin D <20 ng/mL), taking vitamin D supplements reliably raises serum levels and reduces risk of osteomalacia and rickets. Adults often benefit from 800–2,000 IU/day to support calcium absorption and maintain bone mineral density; older adults and people with limited sun exposure or darker skin commonly need higher daily doses or targeted correction regimens.
High‑dose regimens (for example, loading doses given under medical supervision) can correct deficiency faster, and trials such as VITAL used 2,000 IU/day to evaluate broader outcomes; some evidence shows reduced risk of advanced cancer with longer-term supplementation in people without baseline deficiency.
If you already have adequate levels (>30 ng/mL), routine high‑dose supplementation rarely adds measurable bone benefit and may offer limited extra immune protection. Monitor levels if you have obesity, malabsorption, or take medications that affect vitamin D metabolism.
Vitamin D Toxicity and Overdose
Vitamin D toxicity stems from excessive intake of supplements, not sun exposure, and causes hypercalcemia, which can produce nausea, weakness, polyuria, and kidney stones. Toxicity typically occurs with sustained intakes far above recommended ranges — often from chronic high‑dose vitamin D supplements (tens of thousands IU/day) or inappropriate use of high‑dose preparations without monitoring.
Serum 25‑OH vitamin D above ~150 ng/mL raises concern for toxicity; confirm with calcium testing. Treating toxicity centers on stopping vitamin D, restricting calcium, hydration, and in severe cases using bisphosphonates, corticosteroids, or calcitonin under medical care.
Be cautious combining prescription topical agents like calcipotriene (a vitamin D analog) with oral supplements if you have disorders of calcium metabolism; clinicians will monitor calcium and adjust therapy.
Interactions and Special Considerations
Several medications alter vitamin D metabolism: anticonvulsants, rifampin, and certain antiretrovirals can lower levels, while thiazide diuretics raise the risk of hypercalcemia when you take vitamin D and calcium together. If you use calcium supplements or have hyperparathyroidism, coordinate dosing and monitoring with your clinician.
People with obesity often need higher doses to reach target serum levels because vitamin D is sequestered in adipose tissue. Those with fat‑malabsorption (celiac disease, pancreatic insufficiency) may require higher oral doses or injectable/UV strategies.
If you take high‑dose vitamin D supplements, ask your clinician to check serum 25‑OH vitamin D and calcium at baseline and after 8–12 weeks, then periodically. Keep over‑the‑counter dosing within recommended ranges unless a provider prescribes otherwise.



The Healthyish Protocol
Stay connected and follow us on social media for the latest updates!
Express your ideas or propose a topic.
© 2024. All rights reserved.